

Phenibut is not a GABAᴬ agonist
two decades of confusion later


(tl;dr)
Phenibut is a globally consumed depressant, acting as a low-affinity GABAᴮ agonist (around 225 times weaker than baclofen), and more importantly, as a gabapentinoid. A recent case report involving a patient withdrawing from phenibut and bromazolam is one of the many papers mindlessly citing an early 2000s review written by I. Lapin, mistakenly characterizing it as a GABAᴬ agonist:
Phenibut is a glutamate derivative that acts as an agonist predominately on GABA-B receptors, and to a lesser extent, GABA-A receptors.
Due to phenibut’s nonspecific binding to GABA-A receptors, concern for autonomic instability and seizures was prioritized in our case.
Phenibut and Bromazolam Use Disorders Requiring Hospitalization for Medically Supervised Withdrawal
It’s not the first piece of academia citing Lapin for phenibut’s supposed agonist effects at the GABAᴬ receptor - in fact it’s a common misfortune (1 2 3 4).

Izyaslav Lapin was a former Director of Science and Chief of the Bekhterev Psychoneurological Institute between 1960 and 1990. A lab that created and characterized a large majority of obscure Soviet-era GABAergics: phenibut, picamilon, hopantenic acid, faclofen, 2-hydoxysaclofen - the list goes on.
The source appears to be a 2001 review published in CNS Drug Reviews, titled Phenibut (β‐Phenyl‐GABA): A Tranquilizer and Nootropic Drug, in which Lapin simultaneously states that phenibut is a GABAᴬ agonist, phenibut may be a GABAᴬ agonist and that phenibut is not a GABAᴬ agonist.
It acts as a GABA-mimetic, primarily at GABAB and, to some extent, at GABAA receptors.
The degree of certainty at which Lapin presents phenibut as a GABAᴬ agonist only decreases after the abstract. Evidence is presented in the section Putative Mechanisms of the Central Action of PB:
Numerous studies reported activation of GABAB receptors by PB (1,7,8,10,11,35,43,44). In vitro PB binds to bicuculline-insensitive GABAB receptors. In a result typical of GABA-mimetic compounds, direct application of PB to the substantia nigra of rats produced contralateral rotation (38). This effect was not antagonized by bicuculline and suggested that it is mediated by GABAB, rather than GABAA receptors (2,43). However, a secondary activation of GABAA receptors by PB was not excluded. Direct administration of muscimol (an agonist at GABAA receptors) to substantia nigra of rats induces contralateral rotation. PB is also known to cause this effect. Discontinuation of chronic injections of PB to rats increases the density of GABAA and BDZ receptors in striatum while that of GABAB is decreased (38). Chronically administered BDZs have opposite effects.
In this passage plagued by contradictions, Lapin suggests that phenibut may act as a GABAᴬ agonist because direct application into substantia nigra causes contralateral rotation - like muscimol, a well-documented GABAᴬ agonist.
But this test from the stone age reveals little about specific pharmacology, and in fact, the prototypical GABAᴮ agonist baclofen was the first GABAergic to produce the same effect. An identical result is not suggestive of GABAᴬ activity.
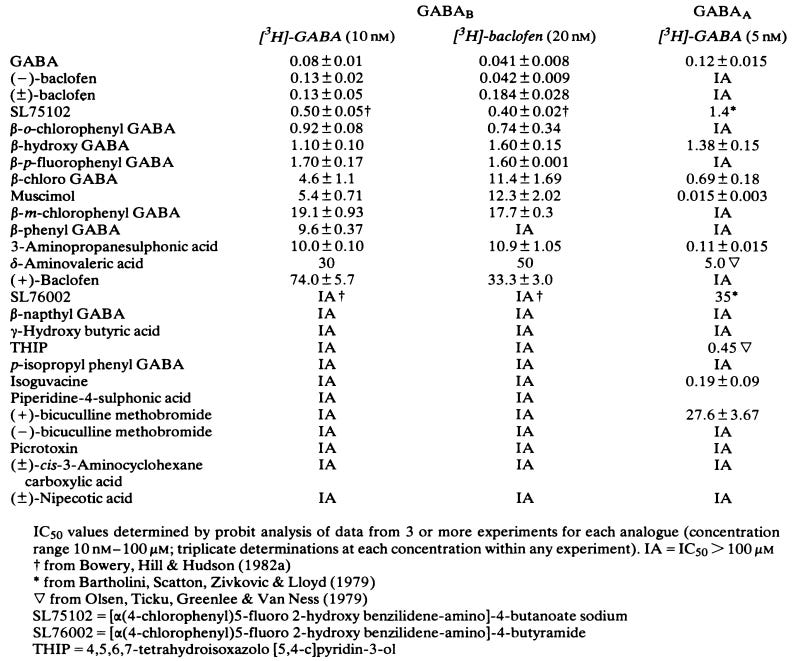
Finally, Lapin provides us with a handy table summarizing results from various studies cited:

In short, Lapin does not provide sufficient evidence to suggest that phenibut is active at the GABAᴬ receptor. Not only does the review mostly cite results from his own lab, the overarching issue is the lack of a binding assay, leading to other misleading or false claims derived from crude qualitative tests (e.g. phenibut as a “PEA antagonist”).
Phenibut was assayed at GABAᴬ in 1983, in which it was found inactive.
A modern assay is still missing as of 2023.
As a takeaway, extreme caution and rigorous fact-checking should be practiced when citing ancient literature for the pharmacology of emerging substances. Failing to do so perpetrates misinformation at best and affects patient outcomes at worst.